
AstraZeneca Brasil came with a clear request: 15 email and hotsite templates to support their medical communications program. No strategy, no system, just templates.
Through our discovery process, we identified that the real problem was structural. The team had no framework for how to communicate with their physician base, no consistency across editorial verticals, and no way to understand whether any communication was actually working. Each send was a one-off. There was no logic connecting email to hotsite, no response to physician behavior, and no path to evolve the communication independently after delivery.
Fifteen templates would have solved nothing. We redesigned the brief entirely. The deliverable became a communication infrastructure with behavioral strategy built in from the start.
We mapped the full communication landscape: what AstraZeneca needed to say, to whom, when, and through which channel. Four distinct editorial verticals emerged, new products, events, articles and content, and public consultations, each with different goals, different physician responses, and different definitions of success.
The critical finding was behavioral. A physician who opened an email but did not click is different from one who clicked but did not interact with the hotsite. Both are different from one who completed every touchpoint. These distinctions were being ignored entirely, every non-response triggered the same follow-up, or none at all.
We mapped every behavioral branch for each vertical and built visual strategy maps showing the full communication arc from initial send through every physician response scenario.
The strategic trails per editorial vertical, and the entire vision of post-interaction response, were not part of the original brief. They were proposed, designed and delivered as a strategic layer AstraZeneca had not envisioned. The team left with not just templates, but a framework for how to communicate with their physician base going forward.
Each vertical received its own communication strategy, trigger logic, content artifact structure and post-interaction path. Four distinct systems sharing the same modular foundation.
Communication strategy. For each vertical, we defined the full arc: initial send, email open tracking, click identification, hotsite access, interaction identification, and a distinct post-communication path depending on physician behavior. Retrigger logic was built for each failure point: no open, opened but no click, clicked but no hotsite interaction, hotsite accessed but no action, and the happy path.
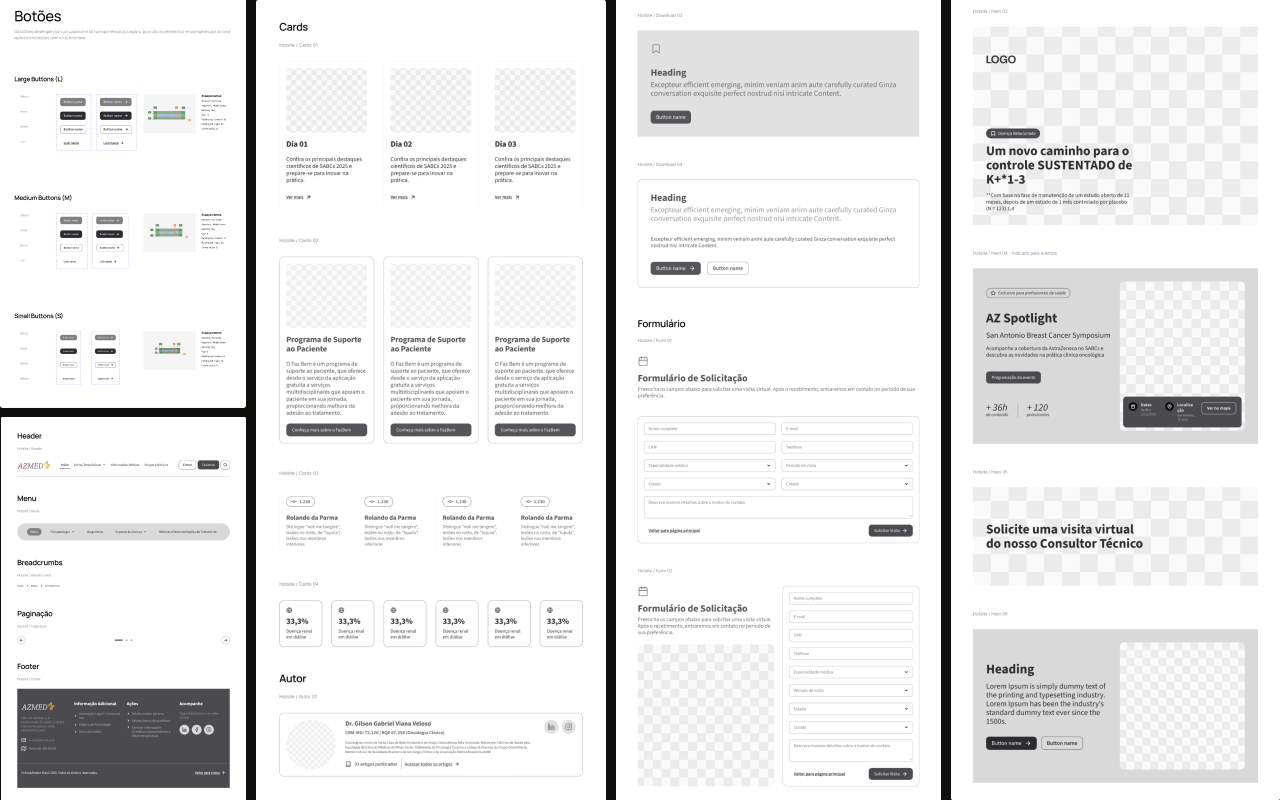
Modular system. We defined the content artifact logic first, author, date, body text, pull quote, comment, CTA, newsletter signup, then mapped which artifacts applied to each vertical and each phase of the communication arc. The system was designed to cover all combinations without requiring new components.
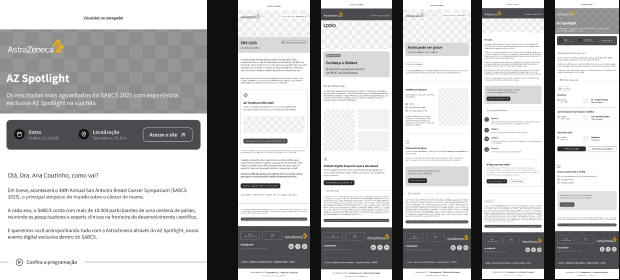
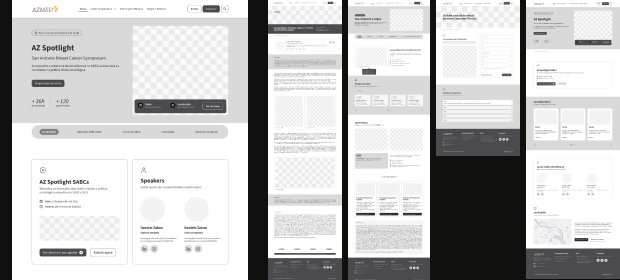
Component library. A responsive modular component library covering all artifact types, built to work across email and hotsite. Each component was designed to combine freely while maintaining visual and structural consistency.
Templates. Using the component library, we built all 15 originally requested templates, now as coherent instances of the system rather than one-off pieces.
Documentation. A usage manual and evolution guide so the internal team could build new templates, adapt existing ones, and extend the system to new verticals without external dependency.
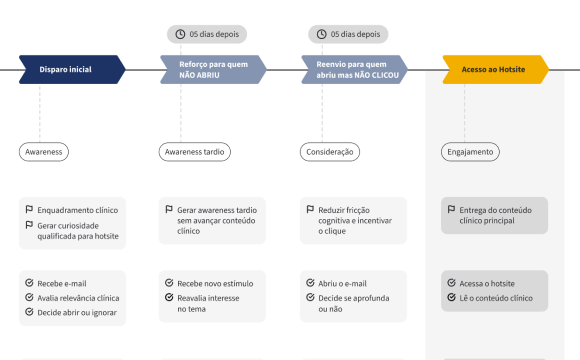
Each behavioral branch had a distinct response. A physician who opened the email but did not click received a different follow-up than one who clicked but did not interact with the hotsite. The happy path triggered a distinct post-communication strategy per vertical. This level of granularity was entirely outside the original brief.